

The chest is home to some of the most vital structures in the human body. The lungs that breathe life into every cell. The heart that drives blood through every vessel. The oesophagus that carries nourishment from one end of the body to the other. The diaphragm that makes every breath possible. When any of these structures is affected by disease, injury, or a condition that cannot be managed with medication alone, thoracic surgery becomes the pathway to treatment, relief, and in many cases, cure.
At Fakeeh University Hospital Dubai, our thoracic surgery programme offers the full spectrum of chest and lung surgical care from minimally invasive video-assisted procedures to complex oncological resections delivered by an internationally trained specialist team with access to the most advanced surgical technology available in the UAE. This comprehensive guide explains everything patients and families need to know about thoracic surgery what it is, which conditions it treats, what procedures are available, and what recovery looks like.
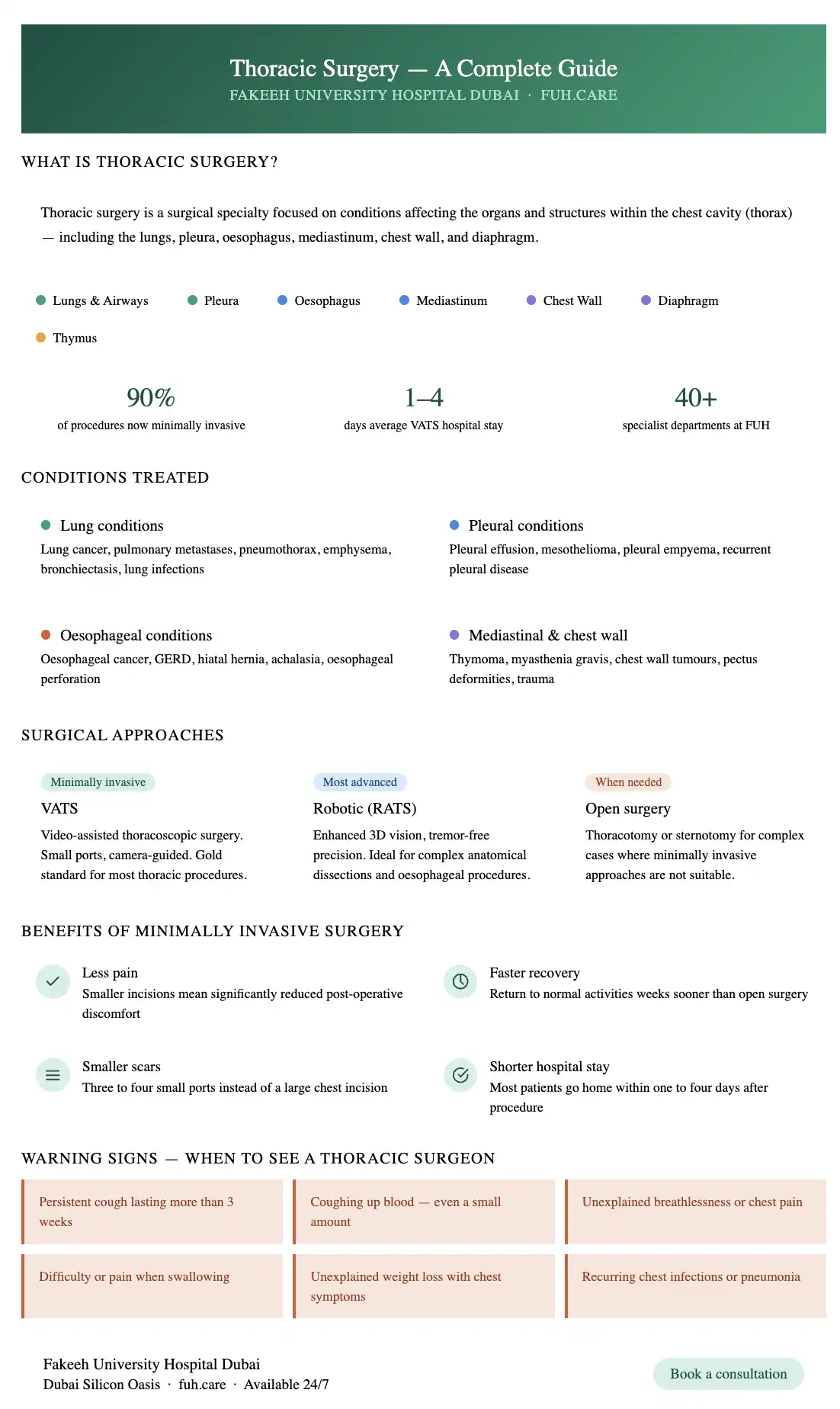
Thoracic surgery is a surgical specialty focused on the diagnosis and treatment of conditions affecting the organs and structures within the chest cavity — known medically as the thorax.
The thorax encompasses:
Thoracic surgery may be performed for cancer, infection, trauma, structural abnormalities, or benign conditions that significantly affect breathing, swallowing, or overall health and quality of life.
Lung cancer is the leading indication for thoracic surgery globally. Surgical resection removal of the tumour along with a margin of healthy tissue and associated lymph nodes offers the best chance of cure for early-stage non-small cell lung cancer (NSCLC). Surgical options range from a wedge resection (removal of a small wedge of lung tissue) and segmentectomy (removal of an anatomical segment) to lobectomy (removal of an entire lobe) and pneumonectomy (removal of an entire lung) the choice depending on tumour size, location, and the patient's lung function reserve.
In selected patients with metastatic cancer that has spread to the lungs from another primary site, surgical removal of lung metastases (pulmonary metastasectomy) can significantly improve survival and quality of life.
Severe lung infections including lung abscess and certain cases of empyema (infected fluid in the pleural space) that do not respond to antibiotics may require surgical drainage or resection.
A pneumothorax occurs when air enters the pleural space, causing the lung to collapse. Recurrent or large pneumothorax is managed surgically through a procedure called pleurodesis or bullectomy removing the air-filled blebs responsible for the leak and sealing the pleural space to prevent recurrence.
In carefully selected patients with severe emphysema, lung volume reduction surgery (LVRS) removes the most diseased, overinflated portions of the lung improving breathing mechanics and quality of life for the remaining healthy lung tissue.
Chronic, irreversible dilatation of the airways causing recurrent infection and symptoms surgical resection of the most severely affected segments may be appropriate in selected cases.
Accumulation of excess fluid in the pleural space between the lung and chest wall can compress the lung and cause breathlessness. Surgical drainage, pleurodesis, or placement of a permanent drainage catheter may be required for recurrent or malignant effusions.
Malignant mesothelioma is a cancer of the pleura most commonly associated with asbestos exposure. Surgical treatment including pleurectomy and decortication plays a role in the multimodal treatment of selected patients.
Infected fluid in the pleural space requiring surgical drainage and, in chronic cases, decortication to remove the thick fibrous peel that restricts lung expansion.
Oesophagectomy removal of part or all of the oesophagus — is the primary surgical treatment for oesophageal cancer. It is one of the most technically demanding operations in thoracic surgery, requiring the stomach or colon to be used to reconstruct the oesophagus after removal.
Severe, treatment-resistant GERD and hiatal hernia where the stomach pushes through the diaphragm into the chest can be corrected surgically through fundoplication or hiatal hernia repair, performed minimally invasively in most cases.
A motility disorder where the lower oesophageal sphincter fails to relax during swallowing causing progressive difficulty swallowing. Surgical myotomy (Heller myotomy) divides the muscular sphincter to restore normal swallowing function.
A rare but life-threatening condition surgical repair is often required emergently.
The thymus gland located in the upper front chest can develop benign or malignant tumours. Thymectomy surgical removal of the thymus is the primary treatment.
An autoimmune neuromuscular condition in which thymectomy has been shown to significantly improve symptoms and disease control even in patients without a visible thymoma.
A range of benign and malignant mediastinal masses including dermoid cysts, lymphomas, and neurogenic tumours may require surgical resection for diagnosis or treatment.
Both primary bone and soft tissue tumours of the chest wall and secondary involvement from other cancers may require surgical resection and reconstruction.
Congenital deformities of the chest wall pectus excavatum (sunken chest) and pectus carinatum (pigeon chest) can cause significant functional and psychological impact. The Nuss procedure and other minimally invasive corrections are now available for eligible patients.
Multiple rib fractures, flail chest, and penetrating chest injuries may require surgical stabilisation and repair.
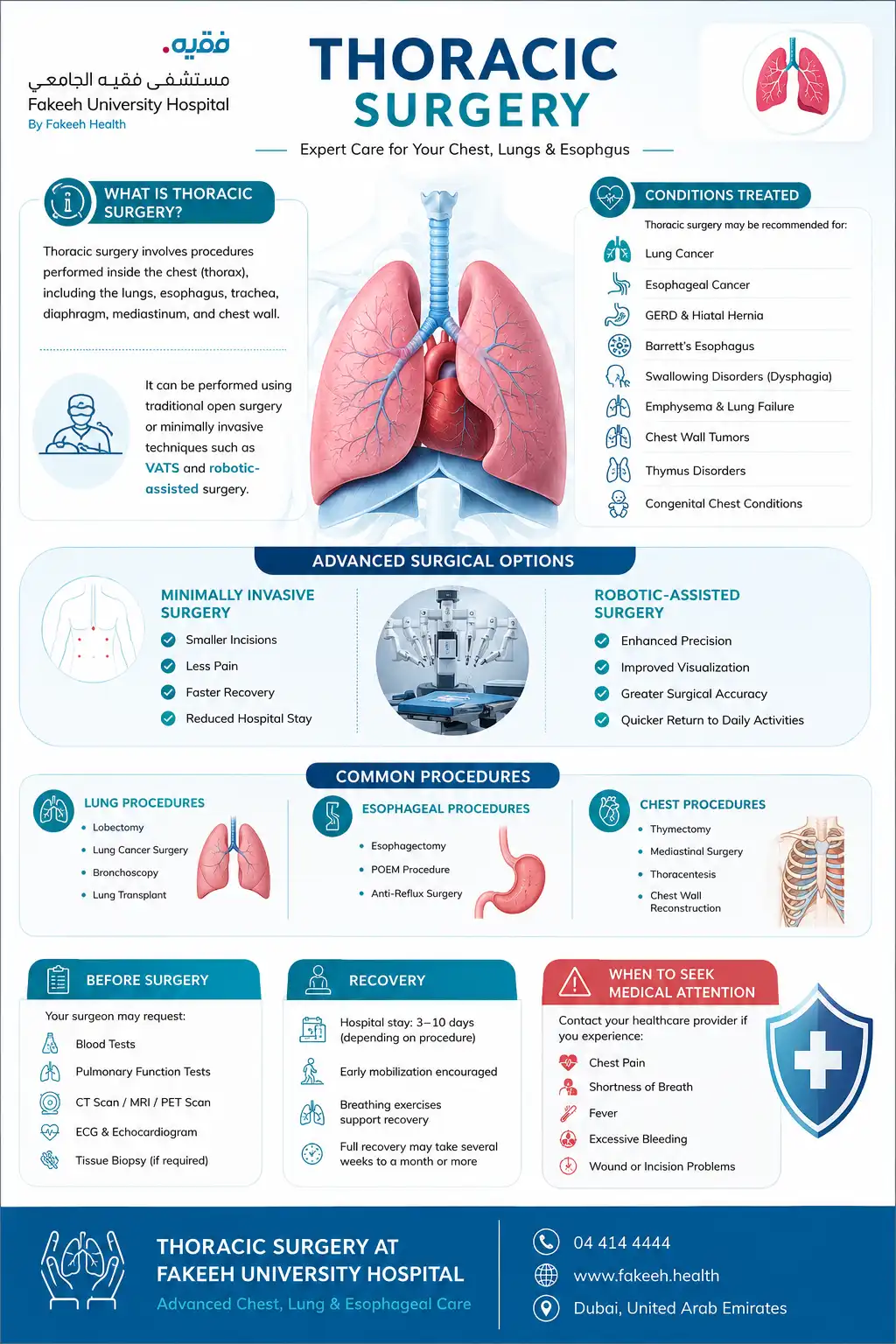
The majority of thoracic surgical procedures are now performed using minimally invasive approaches offering significantly better patient experiences and comparable or superior outcomes to open surgery.
VATS is the gold standard minimally invasive approach for most thoracic procedures. Using small incisions and a thoracoscope a thin camera inserted into the chest our surgeon visualises the entire thoracic cavity on a high-definition monitor and performs the procedure using specialised instruments passed through additional small ports.
Robotic thoracic surgery builds on the advantages of VATS adding the precision, dexterity, and enhanced three-dimensional visualisation of robotic surgical systems. Particularly valuable for complex anatomical dissections, lymph node clearance, and oesophageal procedures. At Fakeeh University Hospital, our thoracic team offers robotic-assisted thoracic surgery representing the most advanced minimally invasive option available for eligible patients.
A thoracotomy involves making a larger incision in the chest wall between the ribs to provide direct access to the thoracic cavity. While minimally invasive approaches are preferred in most cases, thoracotomy remains the appropriate approach for certain complex, large, or anatomically challenging procedures.
A median sternotomy dividing the breastbone is used primarily for procedures involving the anterior mediastinum and is most commonly associated with cardiac surgery, though thoracic surgeons use it for select mediastinal procedures.
A scope is passed through a small incision above the sternum to examine and biopsy lymph nodes in the mediastinum important for staging lung cancer and diagnosing mediastinal conditions.
A flexible or rigid camera passed through the airways used for diagnosis, biopsy, and therapeutic interventions including removal of foreign bodies and management of airway obstruction.
A needle biopsy of a lung nodule or mass performed under CT guidance the least invasive approach to obtaining tissue from a lung lesion for histopathological analysis.
Preparation for thoracic surgery typically begins several weeks before the planned procedure and involves:
Pre-operative assessment:
A thorough evaluation of your overall health, lung function, cardiac status, and fitness for surgery. This includes blood tests, chest X-ray, CT scan, lung function tests (spirometry and diffusing capacity), and an ECG.
Smoking cessation:
If you smoke, stopping at least four to six weeks before surgery significantly reduces the risk of pulmonary complications and improves your recovery. Your surgical team will support you in this.
Pulmonary rehabilitation:
For patients with reduced lung function or those undergoing major lung resection, a programme of breathing exercises and physical conditioning before surgery can meaningfully improve post-operative recovery.
Medication review:
Certain medications including blood thinners, anti-inflammatory drugs, and some supplements need to be stopped before surgery. Your anaesthesiology and surgical team will provide specific guidance.
Nutritional optimisation:
Good nutritional status significantly improves wound healing, immune function, and recovery after major thoracic surgery. Nutritional assessment and support may be recommended for patients with unintentional weight loss or poor appetite.
Recovery after thoracic surgery varies significantly depending on the procedure performed, the approach used, and the individual patient's health and fitness.
In hospital:
Most patients wake from thoracic surgery with one or two chest drains in place tubes that drain air and fluid from the pleural space as the lung re-expands. These are typically removed within one to three days as the lung recovers. Early mobilisation getting out of bed and walking is encouraged from the first post-operative day. Physiotherapy and breathing exercises are an essential component of in-hospital recovery.
Length of hospital stay:
At home:
Pain management, breathing exercises, and gradual return to activity are the foundations of home recovery. Most patients are advised to avoid driving for two to four weeks, heavy lifting for six to eight weeks, and return to full physical activity over a period of four to twelve weeks depending on the procedure.
Follow-up:
Regular follow-up appointments with your thoracic surgeon are essential for wound assessment, monitoring of recovery, and in cancer patients, ongoing oncological surveillance.
Contact your surgical team or seek emergency care immediately if you experience:
At Fakeeh University Hospital Dubai, our thoracic surgery programme combines internationally trained surgical expertise with the most advanced minimally invasive and robotic surgical technology offering every patient the most effective, least invasive, and most personalised surgical care available.





